 Issue PDF
Issue PDFI had the pleasure of investigating the newest and latest versions of anesthesia machines at the 2003 ASA meeting. I was surprised to observe an auxiliary common gas outlet on the Anestar machine (by Datascope), which could easily and perhaps inadvertently be lifted up and opened during mechanical ventilation. This seemed to be possible without indication to the user, and the fresh gas flow would then be diverted into the room. It was my understanding that prior standards for anesthesia machines (ASTM F1850-98a Section 10; 69.2 Note 25 and 69.2.1, Tests for Compliance) required some type of locking device for the common gas outlet to prevent unnoticed or undesirable disconnection from the breathing circuit. Although many of the modern machines have a direct connection of fresh gas to the breathing circuit, the presence of these “auxiliary” outlets (also found in the GE Datex-Ohmeda Aestiva) has recreated the need for a locking mechanism and/or a visual/audible warning.
I must add that I personally spoke to Abe Abramovich, the Director of Anesthesia Systems Development at Datascope, Corp., about this problem, and his receptiveness to an immediate solution encouraged me to co-create this “Dear SIRS” column in the APSF Newsletter. Following is Mr. Abramovich’s response to my concerns. I believe that clinicians and industry can work together in a constructive and professional manner to improve the safety of our patients.
Michael A. Olympio, MD
Chair, Committee on Technology
APSF
Response:
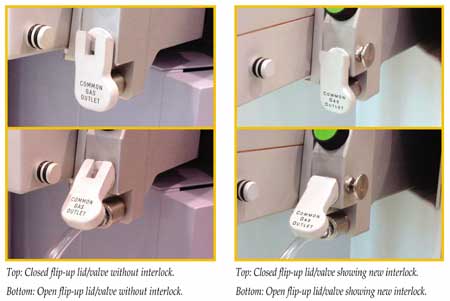
The issue you are referring to regarded the fresh-gas outlet port on the right side of the Anestar’s patient module. In the original implementation, lifting the spring-loaded, flip-up port lid to insert an external circuit connector operated an internal valve which directed the fresh-gas flow away from the circle system to the fresh-gas port. Normally, if an external circuit is NOT inserted into the fresh-gas port, the resting position of the lid/valve is in the closed position and internal gas flow is directed to the circle system. During the last ASA, you observed that a mechanical interlock to the lid/valve would deter unintended actuation of the device. At the time you saw the original implementation, the fresh-gas port had not yet been released to the field. Although not a hazard to patient safety, since the spring-loaded lid/valve ensures valve closure when not in use, Datascope appreciated this suggestion and implemented it. See before and after photographs below. I view such input as one of the positive elements in the APSF relationship between anesthesiologists and industry in exchanging views and ideas. We all have the patient’s best interest in mind, and want the use of Datascope’s equipment to be a positive experience.
Abe Abramovich
Director, Anesthesia Systems Development
Datascope Corp., Patient Monitoring Division
Mahwah, NJ